| AFFECTIVE SYMBOLIC DIS-DIFFERENTIATION: A THEORETICAL MODEL FOR SCHIZOPHRENIC PSYCHOSES |
Souza, G.F.J.*
*Psychiatric Physician
Supervisor for interns at "Hospital das Clínicas" UFMG (Federal University of Minas Gerais)
ABSTRACT :
In this paper the author frames the concept of affective symbolic dis-differentiation in order to propose a theoretical model to elucidate the phenomenological morphology of the psychopathological symptoms of endogenous psychoses, included in the schizophrenia group. Once the concept has been formulated, along with other concepts such as sensorial transformation process (sensorialization) and reification , he makes a careful analysis of KURT SCHNEIDER first-rank symptoms, trying to establish a plausible theoretical sense which would clarify the causes and structure of those anomalous experiences typical of schizophrenia.
KEY WORDS:
Schizophrenia
Affective symbolic dis-differentiation
Sensorial transformation process (Sensorialization)
Reification
KURT SCHNEIDER first-rank symptoms
Psychopathology
INTRODUCTION:
The concept presented here was originally framed in a theoretical essay dated from 1990, under the title of "As Psicoses Endógenas: Uma Visão Fenomenológico-Dinâmica (Endogenous Psychoses: A Phenomenological-Dynamic Approach)"(1). Since then, so far as I have been able to, I have been searching for a similar concept in the specialised publications and, after eight years’ research, it seems not to be there. Nevertheless, even with the present technical resources, such research is not always entirely satisfactory, considering the great number of new papers being published and the possibility that a similar concept has been released during this time. Even so, considering the positive reaction that was given to the afore-mentioned paper by Prof. Alfred Kraus after it was presented in Heidelberg in 1991 by Prof Maurício Viotti Daker, currently Assistant Professor of Psychiatry at UFMG, it is reasonable to conclude that the work possesses some originality. This is all the more so considering that Prof Kraus kindly offered to contribute a preface if the paper were published. Thus, this article intends to define and discuss the concept proposed as well as show its usefulness in the clinical thinking of daily psychiatric practice as a theoretical tool the physician can use to diagnose and understand anomalous experiences typical of schizophrenia.
DEFINING AND DEVELOPING THE CONCEPT:
To start with, considering that thought is formed by a broad association of ideas and representations that are symbolic in nature, a brief theoretical overview would seem appropriate. In another work (2), we already analysed the question of the symbolic differentiation of the human psyche, including the ontogenetic and phylogenetic dimensions. There I formulated the hypothesis of rising symbols, starting from the sphere of sensory perception towards the sphere of intellect, which takes priority in representation. In this regard, we may say that the two basic poles of this movement, that is, the perceptive and the representative poles are the two fundamental kinds of psychic content: the perceptive image and the representative image respectively. We have already proposed (2) the hypothesis that a symbol, when rising up towards the intellect, would gradually lose its original aura of material and concrete sensoriality, and progressively acquire an increasingly more abstract and representative aspect. Stated in other terms, perhaps as a better illustration of this statement, we could say that a perceptive image would have a value of sensorial clarity equal to infinity and an abstract ‘clarity’ equal to zero, whereas a representative image would have a value of sensorial clarity equal to zero and an abstract ‘clarity’ equal to infinity. One usually regards the perceptive image as coming from the external world. Anyone believes, convinced naturally, that those acoustic and optical images he/she perceives are directly related to objects outside him/herself, are linked to facts and events which happened outside himself, and caused by something or somebody else. The sensorial clarity that comes with the experience of those images leaves no doubt about their origin. In contrast, the representative image is regarded as coming from inside our own subjective psyche. When a concept, an personal opinion or a wish are subjectively represented, they are loaded with an inner certainty about the unique identity of those idea producers and affective impressions. The well-delineated subjective boundary between those two worlds, external and internal, constitutes the basis for the individual’s system for judging reality.
We have already discussed (2) the nature of magic thinking and pointed out some analogies between the archaic-magic thinking and a child’s thinking. Apparently, these analogies seem to rely on what we can call inaccurate boundary between the perceptive and the representative images, that is, between reality and imagination. In our opinion, the magic-primitive thinking along with all its peculiar features, such as, the belief in the power to act at a distance, in the power to inflict harm on a hated enemy by damaging parts of an effigy that represents him, in short, the act of imagining, corresponding, with no restrictions, achieving one’s wishes, are a good example of an imprecise boundary between perceptive and representative images. In this case, the abstract symbolic dimension, representative, is still loaded with concrete sensoriality, perceptive, resulting in a subjective conviction of the efficiency of the actions of thought, imagination operating over and above reality.
As long as we accept the definition of symbolic as something which mediates the sensitive providing it with meaning(3,4), it is likely that a highly abstract representative image will contain kinds of compressed sensorial formulas(5), in other words, it will include the original sensorial contents which the symbolic factor managed to mediate completely and progressively. This is quite visible, firstly, in dreams, in which abstract representations develop themselves and then, led by polarization guidelines induced by analogous relations of meaning, fragmentarily condense themselves as sensorialized and reified contents, resulting in the peculiar aspect of dreamlike material. Secondly, and that is what interest us in this work, the psychopathological manifestations of psychotic patients always show this sensorialization and reification trait, presented to the observer and also to the patient in some phases of the disease as weird, bizarre and inconsistent phenomena.
As for the form of primary schizophrenic delusion, we have already mentioned (2) that it could be the result of the dis-differentiation of the symbolic efficacy in mediating the sensorial-perceptive material from the outside world, hence presenting an archaic characteristic typical of those phylogenetically more archaic psychic structures. On the other hand, the extremely variable content of the delusion could be the result of the population of an inside world ¾ recently deprived of symbolic mediation of the senses ¾ by partially symbolised and pre-conscious psychic contents before the onset of the illness, and which now shape and forge a new personal saga taking place in a new, phantasmal, totally reified subjective world. Now when the abstract imaginary reifies itself entirely and takes up part or even all the individual psychic life, the result is that the subjective references related to the clear boundary between the inside and outside worlds are blurred and vanish. Personal desires, longings and fears, which had previously consisted of a group of emotions and subjective representations, are now objectively achieved by a reification process, that is to say, they acquire a character of uncontestable and irrefutable factual reality. The sensorialized and reified development of the intimate existential story, whether desired or feared, happens concurrently with the collapse of the patient’s abstract representative background (symbolic complex corresponding to the entirety of individual consciousness), the exclusive core of his/her inside world. As a consequence, the patient’s subjective conviction is seriously impaired with regard to his/her ability to recognise his/her own actions towards the outside world as truly his/hers. Thus, due to the sensorialization of the patient’s personal abstract representative background, the conviction core, controlling and ruling the individual consciousness over his/her own actions and thoughts, is pulverised and the psychic contents typical of the inside world are transferred to the subjective space reserved for those of the outside world. For a schizophrenic patient, nearly everything comes from ‘outside’, several events and actions are placed outside him: others think for him, inflict thoughts on him, steal his thoughts and so on. Hence the so called outside intervention phenomena, which are psychopathological symptoms that under certain conditions can be a pathognomonic sign of schizophrenic psychosis, come from the sensorialization and consequent reification of the abstract representative personal background and its subsequent transfer to the subjective space for holding the psychic contents from the outside world.
In our opinion, the Jasperian concept (6) of attribute changing of consciousness activity in the ego can be clearly understood in accordance with what we are putting forward. One simply needs to consider the schizophrenic patient as completely at the mercy of his entirely reified psychic contents, complying passively with ‘controls’ and ‘influences’ that he experiences as being imposed from outside himself; and there is nothing that can be done to lighten such stormy experiences. In those cases, there is a clear and deep change of the subjective consciousness of performance and the patient has the irrefutable feeling that, for instance, it is not him who thinks but some force strange to him. He feels a real automaton, and believes his own actions are influenced and controlled by something from ‘outside’, which he usually regards as some extraordinary power. In schizophrenic psychosis, as the symbolic complex corresponding to the entirety of individual consciousness empties and breaks up, its two attributes ¾ the consciousness of performance and the consciousness of existence ¾ are pulverised. The patient’s consciousness of himself as the producer of his own actions and thoughts dissipates, hence his personal conviction of subjective causality is replaced by the reified conviction of objective causality.
The dissolution of the schizophrenic patient’s abstract representative background, which is the same as the deep change of the symbolic complex corresponding to the entirety of individual consciousness, together with its reification and loss of precise subjective boundary between the inside and the outside worlds, can lead to other strange experiences typical of this kind of illness. The representations of ideas, which, in a healthy human being, correspond to important references related to his biographical data, his existential-historical life course, and the fundamental events that structure the uninterrupted line of his consciousness of existence as a singular and indivisible being, are what composes that symbolic complex responsible for the entirety of individual consciousness. So, it is not unusual that when this abstract representative background breaks up, as a consequence, some strange and enigmatic subjective experiences erupt. This is the case of those split personality phenomena(6) which are the most remarkable and characteristic example of changes in the consciousness of the ‘ego’. Similarly, we sometimes find some changes in consciousness of the identity of the ‘ego’, when the patient believes he has turned into new person, or that he has been ‘re-born’ because of the illness. On the other hand, the massive transfer of psychic contents typical of the inside world to the subjective space reserved for those of the outside world leads to experiences that originate in the change of consciousness of the ‘ego’ in opposition to the outside world, that is, the patient feels he is inseparably linked with objects, phenomena and events which are placed somewhere outside himself.
From the clinical point of view, we can notice how the radical transformations in the schizophrenic’s personality happen, often gradually and progressively. In many cases, the patients report a phase of experience, usually followed by a subjective state of intense and vague expectation or even a kind of anxious and upsetting perplexity full of scattered fears and dark suspicions, which is called diffuse delusional mood 6,7). This stage usually precedes the period of definite transformations of subjective experiences, when new anomalous personal experiences, named primary delusion(6,7), emerge and the definite and irreversible instalment of reified conviction of objective causality takes place. We can state that this transitory state is equivalent to the schizophrenic’s gradual and progressive personality impairment, which is characterised by the three fundamental psychic changes mentioned above and listed below to make it easier to understand:
Deep change, or even dissolution, of the
personal representative symbolic background (symbolic complex corresponding
to the entirety of the individual consciousness), which impairs the attributes
of the consciousness of performance and the consciousness of existence.
Loss of the precise boundary between the subjective spaces for holding
the psychic contents from the inside and outside worlds.
Reification of the symbolic exercise, that is, concrete materialization
of the abstract symbolic dimension of psychic life.
The simultaneous confluence of these three basic changes of the patient’s psychic life can help us to understand the nature of the psychopathological symptoms normally shown by schizophrenic patients and which we will carefully examine below:
KURT SCHNEIDER(7) proposed a way of classifying these symptoms by dividing them in two basic groups: first-rank and second-rank symptoms.
The first-rank symptoms consist of the following changes:
· Experiences influencing corporality
· Outside intervention phenomena:
production or subtraction of
thoughts, feelings or
voluntary actions.
· Echo of thought
· Audible thought
· Thought broadcasting
· Thought withdrawal
· Delusional perceptions
· Dialoguing voices and commenting voices
The second-rank symptoms consist of the following changes:
· Delusional inspiration
· Delusional events
· Other pseudo-perceptions
· Perplexity, Strangeness
· Depressive and Euphoric Dysthymia
· Impoverishment of Affective life
It is hardly necessary to point out the importance and usefulness in clinical practice of this symptomatological classification, although we must recognise that finding one or more first-rank symptoms in any given patient in the early stages of the examination, or even isolatedly, does not necessarily imply a diagnosis of schizophrenic psychosis. It is well known, for example, that patients with affective disorder can easily present similar symptoms and that is why a careful observation of the clinical development of the illness is needed and even experimental therapeutic tests with lithium carbonate. In this regard, FROTA PESSOA(9) states that: ‘...according to DSM-III, people with affective disorder can manifest delusions (including paranoid ones, page 187), hallucinations, marked loosening of the association of ideas, poverty of thought, lack of logical sequence in speech and seriously disorganised, catatonic, bizarre behaviour (page 340). And that is not rare; according to the remarkable review by POPE and LIPINSKI (1978), 20% to 50% of cases of affective disorder are followed by such psychotic manifestations, in isolation or in groups ...’.
On the other hand, conversely nearly all the patients with schizophrenic psychosis manifest those first-rank symptoms in the acute phases of the illness. What does this fact really mean?
To begin answering this question, we shall firstly have to examine each of those psychopathological KURT SCHNEIDER first-rank symptoms(7,8), in order to fully understand the intimate nature of those pathological subjective experiences. Our aim is to enable the reader to understand why, in some nosological situations, patients go through subjective phenomena so awkward and strange to the observer and, at first sight, so far away from reality, daily experience and common sense.
To begin the theoretical development, which will lead to the desired understanding, it is necessary to look through the three fundamental psychic changes we have just established (page 05), which are responsible for the causes of the schizophrenic’s subjective experiences. We have stated the third fundamental psychic change in the following words: reification of the symbolic exercise, that is, concrete materialization of the symbolic abstract dimension of psychic life. What does this statement really mean?
Firstly, we will try to understand what the core of a healthy thinking consists of and what are the interactive and dynamic processes involved in its creation. In a healthy person, we can say that thinking is composed of ideas and representations loaded with affection and emotions in a constant and continuous integrating operation, both inductive and deductive in nature. The great variety of ideas and representations fall along two directive axes that as a whole correspond to the entire system of reality judgement. The first axis corresponds to the subjective reality judgement system and the second one to objective reality judgement system. The former refers to intelligible coherence of the sensitive and/or imaginable reality coming from the person’s inside or subjective space, whereas the latter does it for the same psychic contents naturally considered as coming from the outside world. In any case, the person is provided, by the directive action of those two main systems of reality judgement, with the conviction that a given idea is, in the final analysis, abstract, symbolic, and that given sensorial information, in a similar way, comes from the reality of the senses. The subjective conviction, that is, the feeling of a permanent and irrefutable certainty that one is able to distinguish spontaneously and naturally an abstract idea from sensorial data is a fundamental attribute of human psyche, more precisely, of western human psyche.
We outline thus the personal conviction of subjective causality and objective causality. We all know that we are the ones who produce some of our own ideas, feelings and acts, and that some events which happen to us are due to someone else’s actions, that is, because of facts originating in the outside world. We form judgements about ourselves and about others, interpret events happening in the outside world, conceptualise some attitudes and objects, search for meaning relationships among the various things and feelings. In short, we solidly place ourselves in the world.
To summarise, we can say that the thinking of a healthy human being has those characteristics mentioned above. What about a schizophrenic? What are the big differences?
The schizophrenic thinking is essentially reified, that is, full of a concrete animistic-magic symbology. It is probable that with the outbreak of the affective symbolic dis-differentiation process, which we regard as the fundamental characteristic of schizophrenic disorder and whose cause is still unknown, some modes of phylogenetically archaic symbolization emerge and impregnate the superior process of psychic integration of the indelible character of reification. As for the concept of modes of archaic symbolization that we have previously named as symbolic matrices of the phylogenetic evolutive development (2), WILSON has recently proposed, in an important paper (10), a similar concept which he called epigenetic rules (algorithms engraved in the human brain, which structure, limit and condition the individual and cultural variation). In any case, we believe that the partially symbolised psychic contents, and those prevented so far from reaching consciousness, become entirely reified and reach consciousness covered with an animistic-magic character. As a result, the patient subjectively experiences his/her most intimate, hidden desires and fears in a concrete and reified way, in other words, as genuinely real. On the other hand, the loss of the precise boundary between the subjective spaces for holding psychic contents from the inside and outside worlds ¾ we have claimed this to be the second fundamental psychic change in schizophrenic psychosis ¾ favours the pathological experience of concretely imputing to others those same desires and fears, which in psychoanalysis is called ‘projection’ and we call reified conviction of objective causality. In addition there is the fact that affective symbolic dis-differentiation process leads to a progressive sensorialization of those emotional-symbolic complexes experienced by the patient as real and sensitive events, coming from or placed in the outside world. At this point we should distinguish the concepts of reification and sensorialization. We understand reification as a peculiar character with animistic-magic nature, in other words, with concrete symbolism present in delusional judgements. As for the sensorialization process, we see it as the transformation of experiences recognised as abstract into subjective experiences marked with abnormally concrete sensations. Sensorialization and reification are consequences of the affective symbolic dis-differentiation process and make the patient go through sensorialised experiences as genuinely real and absolutely irrefutable. We believe the patient’s sensorialization process of abstract psychic contents is progressive and varies within a range from lower to higher intensity. For instance, the experience of diffusion of thought, that is, the patient’s subjective conviction that everyone knows the meaning of his/her thoughts, should precede the echo of thought and audible thought experiences, as long as the latter reflect a higher degree of sensorialization of abstract contents. Similarly, real hallucinations precede pseudo-hallucinations as the latter correspond to the total sensorialization of abstract symbolic representations. At this point, due to some ambiguity between the concepts of actual hallucination and pseudo-hallucination, in our opinion we should comment and point out some theoretical considerations regarding those two terms. According to JASPERS (11), pseudo-hallucinations differ from genuine perceptions and hallucinations by their lack of corporality. He claims that any perceptive experience resulting from stimulus within the outside objective space should be considered corporeal, even those more tenuous and inaccurate, whereas pseudo-hallucinations should be perceived in the internal representative subjective space, as they are representative and plastic, that is, they are represented by the subject himself. We know that pseudo-hallucinations can happen in certain subjective states, including those regarded as normal. For example, the pseudo-hallucinations perceived with closed eyelids, arise in a widely varied and optically lively way as a great diversity of images and shapes placed in a huge spectrum of colours, shades and configurations. Or even in those cases when there is a ‘internal visualisation’ of a given image, as a result of extreme clearness, clarity and vividness of thinking and representative thought. But what do pseudo-hallucinations of schizophrenic patients mean? For example, one of my patients, a case of long-term paranoid-hebephrenic schizophrenia in advanced chronic phase, insisted that his grandparent’s spirits lived in his throat and would joke, play tricks and insult him through several ‘voices’. The patient pointed repeatedly at his neck and amid unmotivated and foolish laughter would say ‘Can you hear Dr.? ... They are playing with me?...The spirits’ voices...’ After addressing me in this way, he would mumble incessantly, totally aloof from, and indifferent to, all his surroundings. This is only one among several common examples in clinical psychiatry, which are rather long to be described in detail at the moment. However, in our opinion, this means that schizophrenic patient’s pseudo-hallucinations, from the conceptual point of view, should differ considerably from those found in other subjective states, including the one exemplified by JASPERS*(11).
We understand that although the form of the subjective experiences related to pseudo-hallucinations is similar in psychotic and non-psychotic cases, their nature is essentially different in one situation and in the other. Pseudo-representations found in certain non-psychotic subjective conditions are, in our opinion, the result of a low degree of sensorialization of mnemic psychic content, whereas those experienced by schizophrenic patients, mainly as internal ‘voices’, are the final product of the total sensorialization process of the patient’s symbolically abstract psychic contents. Yet, in the first case, pseudo-hallucinations are not at all associated with delusional judgements, while in the second situation it is almost compulsory to link pseudo-hallucinations to such judgements. That is the reason we think a suitable and useful solution for the matter is to use the terms psycho-sensorial hallucinations and psychic hallucinations, proposed by BAILLARGER(11), to replace the relatively ambiguous concepts of real hallucinations and pseudo-hallucinations respectively, since the former concepts would be more precise and strict in describing the phenomenological report of schizophrenic patient’s hallucinatory experiences. In fact, the essence of psychic hallucinations would consist of total sensorialization and reification of what is called pseudo-hallucination in non-psychotic subjective states. The terms pseudo-hallucination or pseudo-perception would be reserved for those psychic phenomena which at no times would be linked to delusional judgements. In this way, we could understand better why psychic hallucinations correspond to the total sensorialization of the symbolised mental contents, whereas in the psycho-sensorial hallucinations there is just a partial sensorialization of them. It seems that in the case of psycho-sensorial hallucinations, the boundary between the subjective space for holding the psychic contents from the outside world and the one for those of the inside space are not impaired and imprecise yet, as it certainly is in the stages of a schizophrenic process where the psychic hallucinations flourish and multiply. Actually, as the disease develops implacably towards the chronic phase and serious mental deterioration, there is apparently a progressive intra-subjectification of the primary delusion, that is, a gradual and significant reduction of the tension between the inside and the outside world, worsening the integrity of the vital contact with reality. It is exactly in this chronic phase of the disease that the clinical reports of psychic hallucinations described by the patients are more common, especially as ‘voices’ coming from inside their heads, ears or other parts of the body and which sometimes take the shape of dialoguing ‘voices’ commenting the patient’s activities, giving orders, imposing actions and thoughts. It is important to point out that, even in those early stages of the disease, the patient can present psychic hallucinations. From our point of view, supported by clinical experience, it would correspond to a gloomy prognosis since such hallucinatory phenomena correspond to the total sensorialization of abstract psychic contents. In general the early stages of a schizophrenic psychosis is when we more frequently find clinical reports of KURT SCHNEIDER psychopathological symptoms (7,8) related to events from the outside world, such as consciousness of vague meanings, experience of placed or the prepared, delusional perceptions as well as psycho-sensorial hallucinations, as we will discuss below. This fact is undoubtedly related to an acute tension between the inside and outside worlds in the early stages of the illness and tends to decrease progressively with the intra-subjectification of the primary delusion in accordance with the loss of the vital contact with reality.
To conclude, we hope this brief account has clarified our concept of gradation of sensorialization intensity of schizophrenic patient’s experiences. This will surely be clearer when represented graphically as follows :
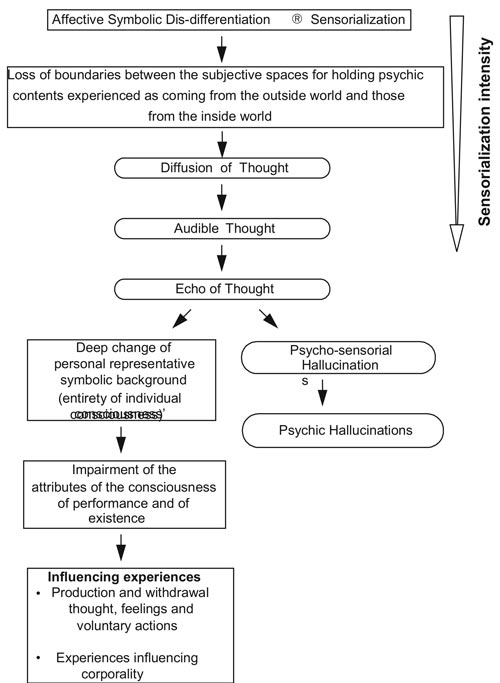
As we can see in figure 01, we have listed those three fundamental psychic changes stated in page 05, responsible for the causes of those experiences typical of schizophrenia and engaged in the production of sensorialised subjective experiences of the disease.
We can see that after the ‘echo of thought’ phenomenon, there is a kind of fork. On the right-hand side of the diagram, we represent graphically the sensorialization process only, leading firstly to psycho-sensorial hallucinations and lastly to psychic hallucinations (process of total sensorialization of abstract symbolic representations). On the left-hand side of the scheme we try to show how the advanced sensorialization process along with the deep change, or even dissolution, of the personal representative symbolic background and consequently of the attributes of the consciousness of performance and of existence, cause the totality of schizophrenic patient’s subjective experiences of influence.
We have also had the chance to frequently observe in clinical psychiatry another kind of phenomenon related to schizophrenic experiences.
On some occasions, the patients only report having gone through a kind of sensorialised subjective experience, like the ones we have just described, without associating any anomalous judgement with this experience. This is what usually happens in the case of those experiences mentioned above, such as, diffusion of thought, echo of thought and audible thought. The patient very often only lives and, puzzled, watches those new and extremely stormy subjective experiences, especially in the early stages of schizophrenic psychosis, without being able to understand precisely what they mean and where they come from. It is reasonable that our psyche, when living an essentially sensorial experience, will regard it as genuinely real and will try to find its source of production in the outside world. However, in a great number of cases, when asked about those kind of experiences, their nature and origin, the patients sometimes answer that they do not know what they mean and where they come from, appearing dazed and confused.
In contrast, on other occasions, usually at the onset and definitive crystalisation of the primary delusion of schitzophrenic psychosis , the patient, with conviction and no doubts, links some judgements to the sensorialised experiences he lives. Thus, for instance, if before the breakout of the illness he was hostile and upset towards his/her neighbour, he is now absolutely and irrefutably sure that neighbour insults him continuously by using bad language and is also ‘stealing’ his thoughts through a fantastic evil machine. We can see clearly how the sensorialization process of the abstract symbolic psychic contents turn into eminently sensorialised experiences ¾ in the referred example, into psycho-sensorial hallucinations, in the form of ‘voices’ the patient believes are uttered by his neighbour and which take up the subjective space for holding the psychic contents regarded as coming from the outside world ¾ which are ‘projected’ onto a given person placed in the outside space. We know that the ‘projection’ psychological mechanism is a physiological psycho-dynamic event which takes place under normal conditions and, predominantly, in situations of neurotic emotional disorders. However, in the schizophrenic’s case, he ‘projects’ sensorialised psychic contents onto the outside world and links them with delusional judgements. In other words, there is a qualitative transformation of the personal conviction of subjective causality into reified conviction of objective causality, the latter consisting of a permanent, irrefutable and crystallised certainty ¾ as opposed to the neurotic’s plastic and flexible ‘projections’ which can potentially develop, dissipate and revert themselves completely at the level of consciousness We believe that besides the several selective ‘projections’ that the patient produces unconsciously, many others are erratically and undeterminedly produced and sensorialised experiences are linked to delusional judgements guided towards nowhere when referring to events and/or people from the outside world. The most classical and outstanding example of those selective ‘projections’, frequently found in daily clinical psychiatry, refers to the patient’s parent figures. It is very common for the patient to develop some hatred, apparently unexplainable, for one of his parents, or even for both. This can sometimes result in tragic consequences and can be explained by the sensorialization of the aggressive emotional contents towards those figures and which is linked with delusional judgements.
After those considerations about sensorialised subjective experiences, we can now classify them in two different categories:
Absolute sensorialised subjective experiences:
these are those sensorialised subjective experiences which are not associated
with delusional judgements, that is, the sensorialised experiences solely
take the place of the immediate experience. For instance, the patients
tells he ‘hears’ his thoughts (audible thoughts), but does not
impute any cause or reason for that. He can not understand the strangeness
of this subjective experience, being puzzled and astonished.
Relative sensorialised subjective experiences: these are those sensorialised
subjective experiences which are necessarily associated with one or more
delusional judgements, that is, the immediate experience’s place
is taken by a two-member experience, the sensorialised component and the
delusional judgements closely related to it. For example, the patient
is convinced that there is an electronic device installed somewhere, which
is imposing and ‘stealing’ his thoughts. Naturally, when the
patient links a sensorialised experience with a delusional judgement,
he is frequently calmer, because at that moment, he builds an intelligible
link within his fantastic logic, which becomes entirely credible to himself
When looking into KURT SCHNEIDER(7) first- and second-rank psychopathological
symptoms, we observe that, concerning events from the outside world, all
those symptoms can be grouped in two classes of different phenomena:
psychopathological symptoms strictly related
to events from the outside world
psychopathological symptoms non-related to events from the outside world.
In the first case, an external stimulus, a given situational circumstance,
in short, a perceptive experience or a set of perceptions triggers one
or more delusional judgements closely related and intrinsically linked
with them. Whereas in the second case, a sensorialised experience takes
the subjective space for holding the psychic contents from the outside
world, that is, it is ‘projected’, mixed and covers the objects
placed in the outside space. And as already mentioned, it can or can not
link itself with delusional judgements related to those same objects.
The first class of phenomena consists of: experience of vague meaning, of "the placed" and of "the prepared" and delusional perceptions.
In the second category are included: diffusion of thought, production or withdrawal of thought, experiences influencing corporality, feelings and actions, psycho-sensorial hallucinations and psychic hallucinations.
We can clearly observe that there is a gradual transition concerning the degree of reification ¾ resulting from the affective symbolic dis-differentiation process ¾ of the delusional judgements in accordance with the increase of the patient’s intimate conviction about the likelihood of the experience in the first group symptoms, that is, those related to events from the outside world.
On the other hand, as for the psychopathological symptoms non-related to events from the outside world, the hierarchical order of the sensorialised experiences, as mentioned above, corresponds to the spectrum of progressive gradation of the intensity of sensorialization, resulting from the affective symbolic dis-differentiation process.
As we have already sufficiently discussed the psychopathological symptoms non-related to events from the outside world, that is the sensorialised subjective experiences, we will concentrate now on those psychopathological symptoms strictly related to events from the outside world.
Experience of vague meaning, which sometimes arises in stage of the diffuse delusional mood, refers to a subjective impression endowed with extreme anxious, indefinite, vague, gloomy expectation established on a significant self-referential background. It all seems to converge towards the patient, gestures, looks, facial expressions acquire a special, singular, slightly threatening aspect. Talks between two strangers seen by the patient from far away turn into audible murmurs and whispers of a slightly discreditable nature about him. He sometimes seems to distinctly hear an insulting word said in a frivolous, insolent way, addressed to him from an inaccurate, undetermined source. Simultaneously, he is struck and overwhelmed by the conviction that everybody can notice the contents of his thoughts in a unexplainable and distressingly intriguing way, and at times he goes through the unusual experience that he is ‘listening’ to his own thoughts. On top of this, in the "experience of the placed or the prepared", when arriving in a place, for example, the patient is immediately overwhelmed by a sudden and irrefutable certainty that some people and/or objects are intentionally placed and arranged with an evil and purposefully declared intent towards him. In short, everything in the outside world moves and shapes itself purposefully and preparedly. The chance occasions of ordinary and trivial daily life turn into facts and actions loaded with specific intention and mysteriously determined purpose in relation to himself. The next stage is the highest degree of reification of the delusional judgements triggered by events from the outside world, which corresponds to delusional perception. In this case, the delusional judgements reach the highest level on the patient’s intimate conviction concerning the likelihood of the experience he lived. For instance, for the patient, a phone call means a sign or a warning he will be murdered. The ‘revealing’, transformation of the world character, as if it were a supernatural, threatening, moving or transcendental message, is rather typical in delusional perception, and is well described by KURT SCHNEIDER (8).
We may observe that, like KURT SCHNEIDER, psychopathological symptoms strictly related to events from the outside world(7), that is to say, consciousness of vague meaning, "experience of the placed or prepared" and delusional perceptions, delusional judgements ¾ in a similar way of the intensity gradation of sensorialised experiences belonging to the group of phenomena non-related to events from the outside world ¾ go through a spectrum of ascending gradation in the patient’s intensity of intimate conviction concerning the likelihood of the experience. In other words, the greater the intensity of reification of delusional judgements, for example in the delusional perceptions, the more crystallised the patient’s intimate conviction concerning the likelihood of the experience becomes.
What we have said so far can
be made clearer if it is graphically schematised as following :
As we can see in the schematic representation of figure 02, the final classification we are proposing for KURT SCHNEIDER’s first-rank phenomena(7,8) implies its dynamic inter-relationship with its three basic characteristics, that is to say: whether linked or not with events from the outside world, gradual intensity of sensorialization of sensorialised subjective experiences and whether delusional judgements are associated or not those same experiences. In the cases of psychopathological symptoms non related to events from the outside world, we have noticed that they correspond to sensorialised subjective experiences represented schematically in details in figure 01. As for psychopathological symptoms closely related to events from the outside world, we found that those phenomena correspond exclusively to the delusional judgements. Moreover, the higher the degree of reification in those judgements the stronger, more powerful and irrefutable the patient’s intimate conviction concerning the likelihood of the anomalous subjective experiences becomes.
These are our ideas about the psychopathological symptoms of schizophrenia. We hope the theoretical concepts presented here will be useful for psychiatrists in general, by adding new approaches for tackling this mental disorder which, despite all progress in neurosciences still remains as a disease of unknown etiology and whose diagnosis is eminently clinical. That is the reason this brief contribution can, to some extent, enlarge a theoretical view able to sharpen and improve our diagnostic sensitivity. If we have achieved that, at least partially, the effort spent on this task will have been worth it.
REFERENCES:
1. SOUZA, G. F. J. "The Endogenous Psychoses: A Phenomenological-Dynamic Approach", , Belo Horizonte, 1990 - Library at Heidelberg University - Germany, (in English)
2. SOUZA, G. F. J. - "Simbolização: Uma Síntese Sócio-Antropológica e Psicológica, (unpublished), 1987. (in Portuguese)
3. CASSIRER, E. - "Antropologia Filosófica", São Paulo, Publisher: Mestre Jou, 1977. (in Portuguese)
4. CASSIRER, E. - "Linguagem e Mito", São Paulo, Publisher: Perspectiva, 1985 - (in Portuguese).
5. KRETSCHMER, E. - "Psicologia Médica", Barcelona, Editorial Labor, 1954 - (in Portuguese)
6. JASPERS, K. - "Psicopatologia General", Buenos Aires, Editoral Beta, l971 - (in Spanish)
7. FERNANDEZ, F. A. - "Fundamentos de la Psiquiatria Actual", Madrid, Publisher: Paz Montalvo,1972 - (in Spanish).
8. SCHNEIDER, K. - "Psicopatologia Clínica", São Paulo, Publisher: Mestre Jou, 1968 - (in Portuguese).
9. FROTA-PESSOA, O. - "Prevalência nas Famílias e Diagnóstico Diferencial das Psicoses", Magazine ABP - APAL, vol. 9, Number 2, 1987 - (in Portuguese).
10. WILSON, E.O. – "Consilience – The Unity of Knowledge", Ed. Alfred A. Knopp, 1998.
11. JASPERS, K. - "Escritos Psicopatológicos", Madrid, Editorial Gredos, 1977 - (in Spanish).
12. AMERICAN PSYCHIATRIC ASSOCIATION - DSM - IV - Manual de Diagnóstico e Estatística de Transtornos Mentais, Porto Alegre, Publisher: Artes Médicas, (4th edition), 1995.
13. BLEULER, E. - "Tratado de Psiquiatria", Madrid, Espasa - Calpe S.A., 1971 - (in Spanish).
14. BUMKE, O. - "Tratado de las Enfermedades Mentales", Barcelona, Francisco Seix - Editor, 1917 - (in Spanish).
15. CHALUB, M. - "Temas de Psicopatologia", Rio de Janeiro, Zahar Editores, 1977 - (in Portuguese).
16. DAKER, M. V. - "Esquizofrenia: Breve Histórico, Conceito e Diagnóstico" - Presented at II Meeting of Brazilian Association of Biologic Psychiatry - November, 1988 - Faculty of Medical Science of Minas Gerais - (in Portuguese).
17 EY, H. - "Estudios sobre los Delirios", Madrid, Editorial Paz Montalvo, 1950 - (in Spanish).
18. HAMILTON, m. - "Abnormal Psychology", England, Penguim Books, 1967.
19. KRAEPELIN, E. - "Lectures on Clinical Psychiatry", New York, William Wood & Company,1914.
20. MILLON, T. - "Teorias da Psicopatologia e Personalidade", Rio de Janeiro, Publisher: Interamericana Ltda. , 1979 - (in Portuguese).
21. SARAIVA, P. - "Delírio Depressivo", Magazine of the Medical Association of Minas Gerais, Belo Horizonte, 35:25 - 7, 1984 - (in Portuguese).
22. SARAIVA, P. - "Parafrenia, Paranóia, Reação Esquizofrênica: Mitos ou Realidades"? Belo Horizonte, Magazine of Galba Velloso Study Centre, Year I, Number 3, July/Sep 1970 - (in Portuguese)
23. SHADER, R. I. - "Manual of Psychiatric Therapeutics", Boston, Little, Brown and Company, 1982.
24. SOUZA, G. F.J. - "Considerações gerais sobre as Neuroses: Uma Visão Fenomenológico-Dinâmica", (unpublished), 1988 - (in Portuguese).
25. VON GEBSATTEL, V. E. F. - "Antropologia Médica", Madrid, Ediciones Rialp, 1966 - (in Spanish).
Author’s mailing address:
Gustavo F. Julião de Souza
Rua Grão Mogol, 698/102
Bairro Anchieta, Belo Horizonte – M.G.
CEP:30310-010
Brazil
E-mail: gustavo1@gold.com.br